March 2022
3/25/2022 | BY Cheryl R. Lawing, MD
5 Tips for Caring for a Child with Down Syndrome
- Consider the entire spine
Scoliosis and spondylolisthesis are also present at an increased frequency in Down syndrome but can be managed similar to idiopathic patients with regard to bracing and surgery indications.
A.
 B.
B. 
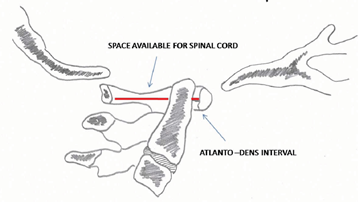
A. Illustration showing the ADI, which should be < 10 mm, and the SAC, which should be > 14 mm. B. Neutral upright lateral cervical spine radiograph demonstrating atlantoaxial instability.
- Consider the hips
A.

 B.
B. 

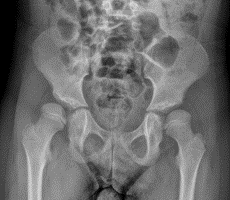
A. AP Pelvis of an 8 yo girl with T21 with bilateral hip subluxation. B. In the two months that it took to arrange her preop CT, her dysplasia progressed to dislocation. In some children, habitual dislocation can occur.
Hypothyroidism is not uncommon in Down syndrome and this is thought to result in the increased incidence of slipped capital femoral epiphysis (SCFE). Differential diagnosis for gait abnormalities, especially in combination with hip or knee pain should include SCFE, though myelopathy should also be considered with gait changes.
- Consider the knees
Patellofemoral instability, which is present in around 1/3 of patients with T21, is common due to the severe ligamentous laxity. This is sometimes associated with genu valgum. Treatment decisions are made on level of symptoms and ranges from bracing to surgery. Physical therapy is often limited due to developmental delays.Lateral release is unlikely to be helpful, whereas medial reefing and distal realignment procedures tend to be more helpful. If genu valgum is present, this may need to be corrected.

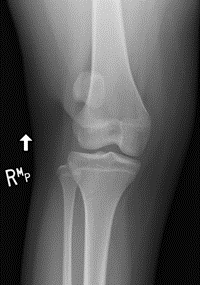
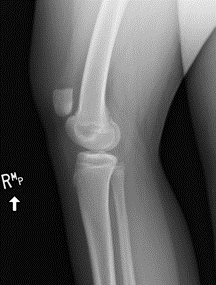

15 yo girl with T21 with right patellar instability. Patella alta noted with lateral subluxation present at baseline. Genu valgum contributes to her instability.
- Consider the foot
A.

 B.
B.

A. Foot radiographs of a 12 yo girl with T21. Hallux primus varus is noted on the standing AP view and the standing lateral (B) shows a negative sagittal Meary’s angle, typical of flexible pes planovalgus.
- Consider the co-morbidities
- Approximately 50% of children with Down Syndrome have congenital heart defects, which are important to be aware of prior to surgical considerations/discussions. This most commonly takes the form of atrioventricular septal defects, ventricular septal defects, persistent ductus arteriosus and Tetralogy of Fallot.
- Leukemia is more common in these children and you should have a low threshold of checking a CBC for fatigue or unexplained pain symptoms.
- Down syndrome associated arthritis is an inflammatory condition affecting children that typically manifests with polyarticular pain and swelling. Similar to JIA, it tends to be seronegative for typical markers such as ANA or RF.
- Premature aging can occur, including high incidence of degenerative joint disease and Alzheimer’s dementia. As care for people with T21 has improved, life expectancy has increased with life expectancy of 60 years. As a result, the functional limitations of this premature arthritis and arthritis related to hip subluxation is more profound.