Study Guide
Femoral Neck Fractures
Key Points:
- Rare injuries associated with high energy and polytrauma
- The Delbet classification is widely used, includes 4 types, and is prognostic for the potential for avascular necrosis
- Treatment is urgent and tailored to the fracture type and patient age
- Complications associated with these fractures are osteonecrosis, nonunion, and premature physeal closure
Description:
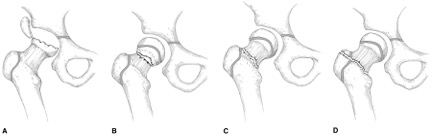
Fractures of the femoral neck and includes fractures that involve the proximal femoral epiphysis, femoral neck, and intertrochanteric region of the femur.Delbet classified femoral neck fractures into four types that provides guidance for treatment and prognosis (Figure 1):
Type 1--transepiphyseal fractures
Type 2--transcervical fractures
Type 3--cervicotrochanteric fractures
Type 4--intertrochanteric fractures
Epidemiology:
Femoral neck fractures account for <1% of all fractures in pediatric patients and <1% of all hip fractures (Canale 1977, Boardman 2009, Ratliff 1962).Clinical Findings:
These patients are unable to bear weight on the injured extremity. They may have a shortened and externally rotated extremity, and the fracture may be associated with other polytrauma injuries (head injuries, abdominal injuries, etc).Imaging Studies:
Plain radiographs are the primary imaging modality to diagnose and classify a pediatric femoral neck fracture. When attempting a cross-table lateral radiograph, care should be taken to move the uninjured limb so as not to significantly displace the fracture on the injured side. CT or MRI may play a role in concurrent femoral neck fracture-dislocations to better define the pattern of injury.(Lee 2010)Treatment:
Treatment ranges from closed reduction and spica casting to open reduction and internal fixation. Capsulotomy has been recommended to evacuate the intracapsular hematoma and potentially decrease the risk of AVN. Treatment is determined by the Delbet classification, displacement, and the age and size of the patient.Type 1 Fractures (Transepiphyseal)
- Closed reduction and spica cast immobilization
- Considered for nondisplaced or minimally displaced fractures up to age 4 years
- Internal fixation
- Appropriate for older children or with displaced fractures
- Closed reduction or open reduction is performed to achieve anatomic alignment
- Smooth pin fixation may be acceptable for small, young children when supplemented with a spica cast
- Cannulated screw fixation is appropriate for older children and adolescents
- Closed reduction and spica cast immobilization
- Considered only for nondisplaced or minimally displaced fractures up to age 4 years
- Internal fixation
- Appropriate for older children or with displaced fractures
- Closed reduction or open reduction is performed to achieve adequate alignment
- Smooth pin fixation may be acceptable for small, young children when supplemented with a spica cast
- Cannulated screw fixation is appropriate for older children and adolescents
- Crossing the physis may be necessary to achieve adequate fixation
- If the fixation stops short of the physis, spica cast immobilization should be considered
- Closed reduction and spica cast immobilization
- Nondisplaced or minimally displaced fractures up to age 3-4 years
- Cross-sectional imaging may be necessary to confirm that reduction is adequate and maintained within the cast
- Closed reduction, pin fixation, and spica cast immobilization
- May be considered for children up to age 6 years
- Rigid internal fixation
- Consider for displaced fractures in children greater than age 3 years
- Closed reduction or open reduction via anterolateral approach
- Proximal femoral plate or compression hip screw
weightbearing within 2 weeks.(Swiontowski 2009)
Complications:
Avascular Necrosis
Rates range from 0-92%.(Riley 2014) A meta-analysis found an osteonecrosis rate of 38% for Type 1 fractures, 28% for Type 2 fractures, 18% for Type 3 fractures, and 5% for Type 4 fractures.(Moon 2006) Another recent study of 44 patients showed rates of 50%, 28%, 8%, and 10% for fracture types 1-4, respectively.(Riley 2014)Delayed union/Non-union
Delayed or nonunion may be related to treatment method. Internal fixation is preferred, when possible, and can reduce nonunion rates.(Bali 2011) The reported incidence is 1-10% of fractures.(Boardman 2009) Subtrochanteric valgus osteotomy without the need for bone graft converts the force across the fracture from shear to compression and is the preferred treatment for femoral neck nonunions.(Canale 1977)Premature Physeal Closure
This may not cause significant limb length inequality due to the robust nature of the distal femoral physis, however the magnitude of the discrepancy will depend upon the age of the child at the time of the physeal arrest.(Hamilton 1961) Physeal closure may be caused by the injury or due to fixation that crosses the physis. A partial growth arrest may cause coxa vara or valga.Related Videos:

References:
- Bali K, Sudesh P, Patel S. Kumar v, Saini U, Dhillon MS. Pediatric femoral neck fractures: our 10 years of experience. Clin Orthop Surg. 2011;2(4):302-8.Epub 2011 Dec 1.
- Boardman M, Herman M, Buck B, Pizutillo P. Hip Fractures in Children. JAAOS. 2009;17:162-173.
- Canale ST, Bourland WL: Fracture of the neck and intertrochanteric region of the femur in children. J Bone Joint Surg Am. 1977;59:431-443
- Hamilton CM. Fractures of the neck of the femur in children. JAMA 178:799-801. 1961.
- Lee DH, Park JW, Lee SH. A transepiphyseal fracture of the femoral neck in a child with 2 widely displaced Salter-Harris III fragments of the capital femoral epiphysis. J Orthop Trauma. 2010;24(2):125-9.
- Moon ES, Mehlman CT. Risk factors for avascular necrosis after femoral neck fractures in 242 children: 25 Cincinnati cases and meta-analysis of 360 cases. J Orthop Trauma. 2006;20:323–329.
- Ratliff AH. Fractures of the neck of the femur in children. J Bone Joint Surg Br. 1962;44-B:528-42.
- Riley PM Jr, Morscher MA, Gothard MD, Riley PM Sr. Earlier time to reduction did not reducte rates of femoral head osteonecrosis in pediatric hip fractures. J Orthop Trauma. 2014 Sep 2. [Epub ahead of print]
- Swiontkowksi MF. Fractures and Dislocations About the Hip and Pelvis. In: Green NE and Swiontkowksi MF, eds. Skeletal Trauma In Children. 4th ed. Philadelphia, PA: Saunders; 2009: 355-396.